
Clinical transplanatation of a tissue-engineered airway
Paolo Macchiarini, Philipp Jungebluth, Tetsuhiko Go, M Adelaide Asnaghi, Loyisa E rees, Tristan A Cogan, Amanda Dodson, Jaume Martorell, Silvia Bellini, Pier Paolo Parnigotto, Sally C Dickinson, Anthony P Hollander, Sara Mantero, Maria Teresa Conconi, Martin A Birchall
Introduction: Patients with end-stage airway diseases often require a replacement of more than 30% (6 cm) of the bronchus length and must seek a full transplant to restore airway function. Replacing the airway is difficult and requires a matrix seeded with cells that exhibit similar mechanical properties to the original tissue and do not generate an immune reaction.
Background: A 30 year-old woman initially diagnosed with tuberculosis and subsequent airway stenosis was treated with antibiotics and a surgery that involved a stent to help keep the airway open. Despite replacement and repositioning, pneumonitis, cough, and mucus persisted. Eventually the stent was removed and the patient developed severe dyspnoea that left her unable to perform even simple tasks. Her lung tests were highly abnormal and doctors suggested a left total pneumonectomy, a procedure with high risk and long term morbidity. Instead, researchers proposed a complete resection of the left main bronchus and replacement with a bioengineered one.
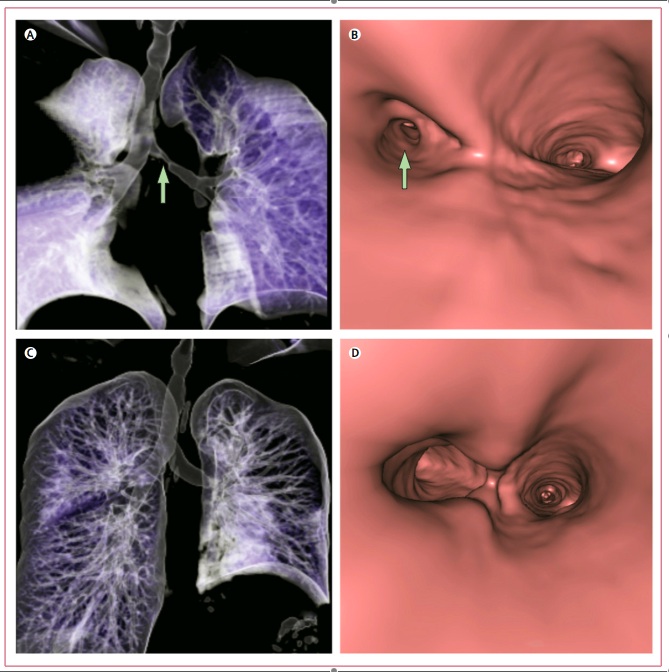
Figure 1: Volume-rendering CT of the bronchoscopic reconstruction before (A&B) and after (C&D) engraftment.
Materials and Methods: A 7 cm trachea from a deceased 51 year-old, type O negative female was removed. It was then placed in PBS containing antibiotics. This was followed by 25 cycles of a decellularization protocol that took six weeks. After each cycle, tests were performed to check for multihistocompatibility complexes (MHCs) and cells to avoid triggering an immune response post implantation. Typically MHCs were detected using a primary anti-human antibody and cells were counted using a DAPI nuclei stain.

Figure 2: Immunostaining of the grafts at retrieval from the patient (A&B), after 17 cycles of washing (C&D), and 25 cycles (E&F). Brown color indicates presence of MHC class 1.
Autologous epithelial cells were obtained from the patient via biopsy from the right main bronchial mucosa. These cells were then cultured in PBS with antibiotics for 2-3 days. The cells were then spun down and resuspended in media in 25 cm2 flasks. Immunofluorescence was used to confirm cytokeratins, an indicator of epithelial phenotype.
Autologous chondrocytes were obtained from bone marrow aspirate that was also treated with antibiotics and then added to media. After centrifugation, the pellet, containing mesenchymal stem cells, was resuspended in complete media. Cells were incubated for three days to promote adherence.
A novel bioreactor was created to allow cells to seed on a scaffold that would become a bronchus. This bioreactor rotated the isolated airway matrix around a longitudinal axis much like a rotisserie. A bath of media compatible with both cell types was filled so that the rotating airway was exposed to media half of the time and air the other half. All of this was contained in a polysulphone chamber rotated by a motor.

Figure 3: The bioreactor setup used to recreate airway tissue conditions.
Cells were first detached from their flasks using trypsin and then diluted to a final concentration of 1 million cells per milliliter. Cells were applied longitudingally to the matrix with a microsyringe. Chondrocytes were seeded onto the external surface and epithelial cells were seeded onto the internal surface. The motor was then turned on, and the seeded bronchus was rotated at a rate of one revolution per two hours. Media was changed once a day for four days.

Figure 4: Color immunohistochemistry of primary bronchial cells at first passage (A), cells from the outer surface of the matrix preimplantation (B), and cells from the luminal surface of the graft 4 days post implantation (C). Epithelial cells appear red and chondrocytes appear green.
To implant the bronchus, the patient’s left main bronchus was removed. The new bronchus was cut to shape and inserted end-to-end proximally and distally. The left recurrent and phrenic nerves were then reconnected and ventilation was restored as the lung filled.
Results and Discussion: 10 days later the patient left the hospital and post-surgical bronchoscopy revealed that there were no complications and that the patient’s lung function had returned to normal. After four days it was noted that the graft was almost indistinguishable. The patient has since been able to go on walks and lead a more normal life.
The success of this procedure indicates that repetitive decellularization cycles can be used to produce allogeneic scaffolds that successfully avert immune rejection. It also indicates that there are ways to reproduce difficult environments, such as that of the air-liquid interface encountered by the bronchi, outside of the body for use in creating viable grafts. It further shows that cells can be co-cultured to recreate the composition of tissues found in the body through strategic seeding and the presence of an allogeneic matrix that helps direct their growth.
Critique: Overall, these researchers did an excellent job establishing a functional protocol for replacing a bronchus when few other options are available to the patient. Their attention to immune rejection and the conditions necessary to simulate the environment of the bronchus led to a successful design that was able to greatly improve the patient’s quality of life. My main criticism is the lack of background research. Although research was performed in pig and mouse models, studies implicating the success of such a procedure in primates are typically performed before they are performed in humans.
In the future, more stringent tests to ensure immune compatibility should be performed. Additionally, more trials to indicate the viability of this method and prove that these results were not unique are required. In addition, this technique of decellularizing a matrix, removing its antigenic components, and then reseeding cells should be applied to explore the replacement of other tissues in the body.
![]()
5 comments:
I found this paper to be very interesting, especially in regards to the use of a bioreactor which is able to sustain the development of two types of cells which needed different culture conditions. The authors did a good job of ensuring that immune rejection would not compromise the transplantation by measuring the presence of antibodies throughout the experiment. While the authors ended up using cells from a biopsy of the bronchial mucosa, it would be interesting to see whether or not cells from other sources or other cell types are able to repeat the results. Since the authors could not determine if the cells on the graft were from growth of seeded cells or growth of adjacent cells, it may be helpful to design in vitro experiments to answer this question. This would allow researchers to determine the components which are necessary for a successful transplantation, whether or not that includes cells. Furthermore, the patients should be followed over a longer period of time to examine whether or not the biomechanical functions of the lung are still optimal.
It is very interesting to see novel bioengineering technology applied in a real clinical setting. The authors did a good job monitoring the levels of immune response throughout the procedure. I agree with the previous poster in that it would be very interesting to see how this procedure holds up in the long term. I wonder how would the success of this procedure look if we followed the patient for a span of several months or even years. It would also be interesting if the authors could provide some more concrete, detailed background of how the novel procedures compares with a total pneumonectomy (i.e. numerical morbidity rates and risks)
This paper is really interesting and fascinating. However, it did seem somewhat worrying that the authors had done this step without other trials beforehand, and the experimental procedure may have lead into some ethical questions. Observation of the woman for longer than the mentioned 10 days would also be desirable, not only to check for full functionality of the implanted airway, but also the chance that there may later be some sort of adverse effect from the engineered airway as a result of using another's matrix, though hopefully this is close enough across individuals. If this, however, proves to be a successful procedure, then there are many other applications for which this will be worth exploring with.
The authors did go through many careful steps to make sure that immune rejection does not occur. They also created various steps to seed different cells in the scaffold to ensure integration into the body. Although this is a successful case, I do wonder if result is replicable. I agree with Ash in that animal studies should have been done first before human implantation. As most people mentioned in the comment, I also believe that the patient should be remain under observation over a much longer period of time. I wonder whether grafting a decellularized bronchus will result in complication in the anastomosis site over a longer period of time (like hyperplasia with grafted blood vessels).
I applaud the researchers in a successful transplantation for a patient that seemed to have no other way of surviving. Although I agree partially with other posters that there should have been more background research and animal testing, there is also the ethics of performing novel experimentation on a dying patient. If the patient consented to this graft as her last option, this is an excellent way for bioengineers to directly apply tissue engineering (since this is the eventual goal of research anyway).
Although people suggest that the patient was not monitored for more than 10 days after the surgery, this may be a misleading conclusion from the paper. It is possible that the paper was published a short time after the transplantation and that subsequent checkups were probably performed.
My main critique is the continued testing of their bioreactor over a longer period. In vitro testing of the bioreactor over an accelerated timeline should be performed to check if there the engineered scaffold will properly degrade over time. Otherwise this could result in problems for the patient later on. The researchers should not only repeat this experiment in a lab setting, but also test the efficacy of their research in several conditions, especially over a prolonged period of time.
Post a Comment